In total, 34 decision trees were developed, driven by 101
decision nodes based on the guideline recommendations.
Decision trees represented recommendations for diagnostics, staging, primary treatment, pathology, and
follow-up and included one overview decision tree for
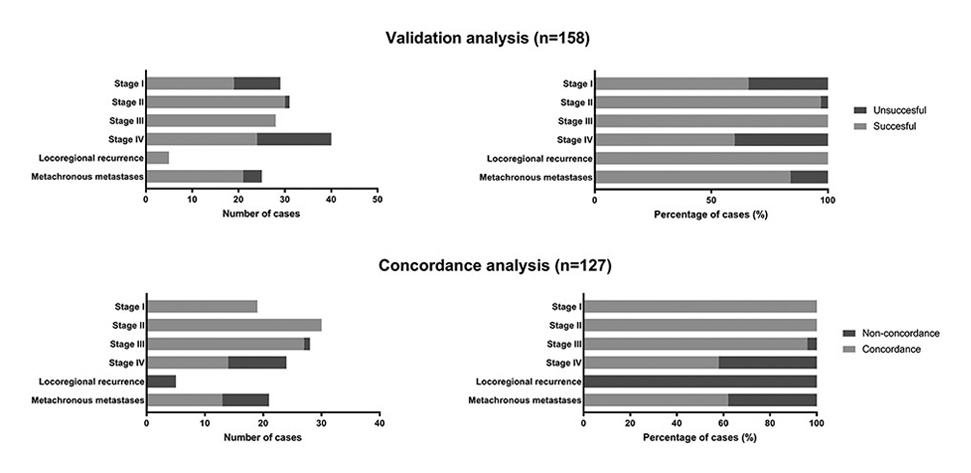
optimal navigation. We identified several guideline information gaps and areas of inconclusive evidence. A total of 158 patients’ MTB reports were eligible for decision tree validation and resulted in treatment recommendations in 80% of cases. The concordance rate between decision tree treatment
recommendations and MTB advices was 81%. Decision trees reported in 22 out of 24 non-concordant cases (92%) that no guideline recommendation was available.



{kind=link}
{kind=link}